

Would Walter White Still Cook Meth in 2025?
Or: How Modern Oncology and Employer Insurance Would Have Ruined the Entire Premise

 receives chemotherapy as his wife Skyler (Anna Gunn) looks on in an episode from the first season of \"Breaking Bad.\"")
You know what’s a fun way to spend a morning? Calculating whether a fictional chemistry teacher’s cancer would be treatable with modern targeted therapy and whether his employer health plan would cover it. I have done this. Let me tell you what I learned.
The basic facts, if you never watched Breaking Bad: A high school chemistry teacher gets lung cancer, has inadequate insurance, cooks meth to pay for treatment and leave money for his family, becomes increasingly murderous drug kingpin, etc. The financial crisis is the inciting incident. Without it - no cancer bills, no blue meth, and no “I am the one who knocks.”
But it’s been 17 years since the show first aired, and cancer therapy has come a long way since. Things have gotten dramatically better since 2008. And re: teacher health insurance -- it was already pretty good in 2008, and it has arguably gotten more standardized and predictable since then, even if not necessarily more generous.
OK, here we go.
The Oncology
In the show, Walter White is diagnosed with stage IIIA non-small-cell lung adenocarcinoma. In 2008, this was essentially a death sentence with palliative care. The five-year survival rate was maybe 15-20% (1, 2, 3). You’d get some chemotherapy and radiation, feel terrible, and probably die within two years.
But in 2025, Walter would immediately get next-generation sequencing of his tumor. Of the population of 50-year-old never-smokers with lung adenocarcinoma, roughly ~30-40% have EGFR mutations (1, 2) another ~10% have ALK rearrangements (1, 2), and maybe 10-15% have other “targetable drivers” (ROS1, RET, MET, etc.).1
Let’s say Walter tests positive for an EGFR mutation, which is the single most likely scenario. His treatment would be:
Concurrent chemoradiation (same as 2008, terrible but manageable)
Then 80mg of osimertinib (brand name Tagrisso) once daily, potentially for years
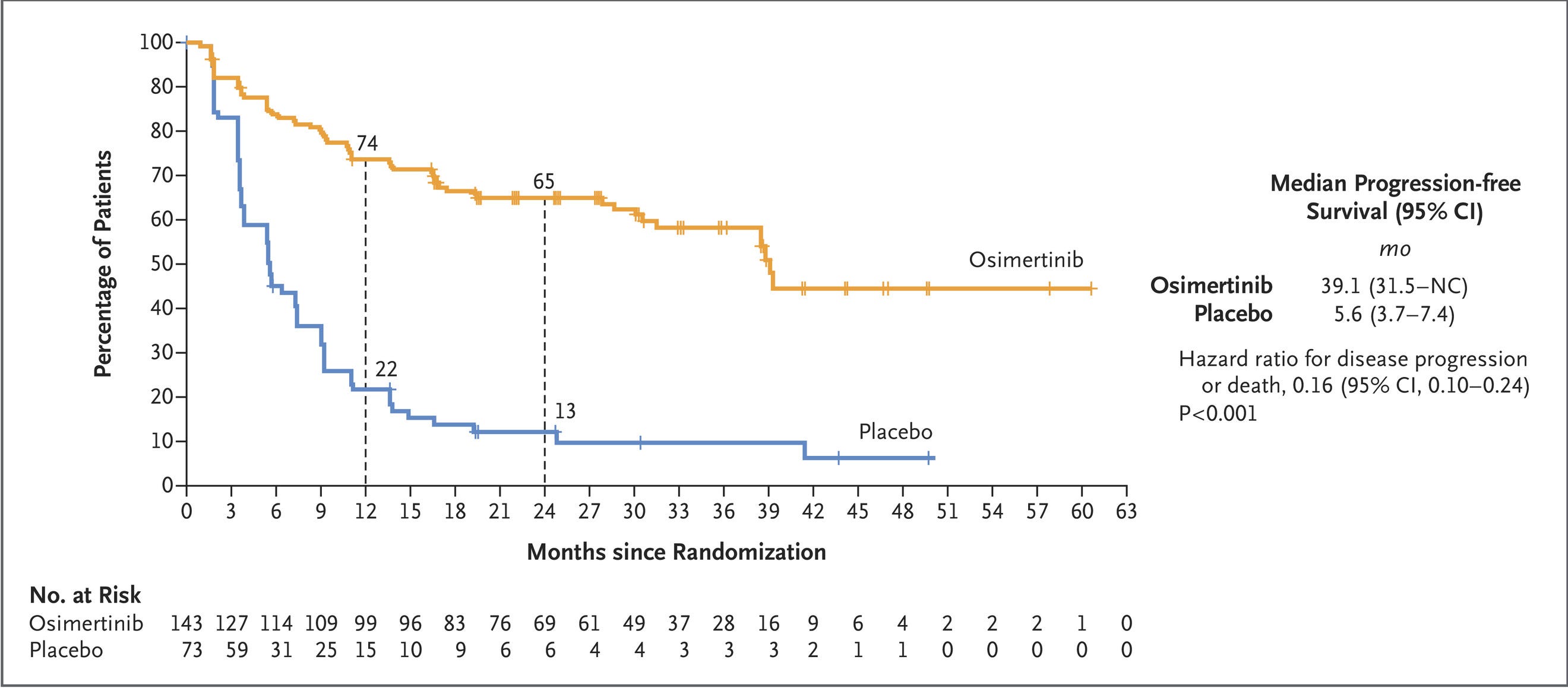
With this course of treatment, his prognosis would be much better than what was available to him in 2008! The LAURA trial, which led to FDA approval in September 2024, showed a median progression-free survival of 39.1 months on osimertinib versus 5.6 months on placebo. That’s a hazard ratio of 0.16. Overall survival data are still maturing, but the trend is strongly positive. The five-year survival for Walter’s profile could plausibly be on the order of 50-60%, versus 10-15% in 2008.
Even if he’s driver-negative, he’d get durvalumab immunotherapy after chemoradiation, which pushes five-year survival from about 33% to 43%.2
So: Walter would go from “you will almost certainly die within two years” to “you have a serious cancer but a realistic chance of seeing your kids grow up.” This is a different show.
The Insurance
In the show, Walter has an Health Maintenance Organization (HMO) plan through Albuquerque Public Schools. When Skyler finds a “top-rated oncologist,” the doctor is out of network. The HMO won’t cover it. The billing office wants $5,000 upfront. Walter balks, then pays with meth money.
Here is what people misremember: The $5,000 is not his deductible. It’s a deposit for an out-of-network doctor that his HMO already declined to cover. Walter chose to go outside his network, probably because he thought he was dying and wanted “the best.”
What would his actual in-network coverage have looked like in 2008? For a large public employer with an HMO:
80% of enrollees had no general annual deductible for single coverage
Among those with deductibles, the average was $307 for large firms
Teacher unions typically negotiated better-than-average benefits
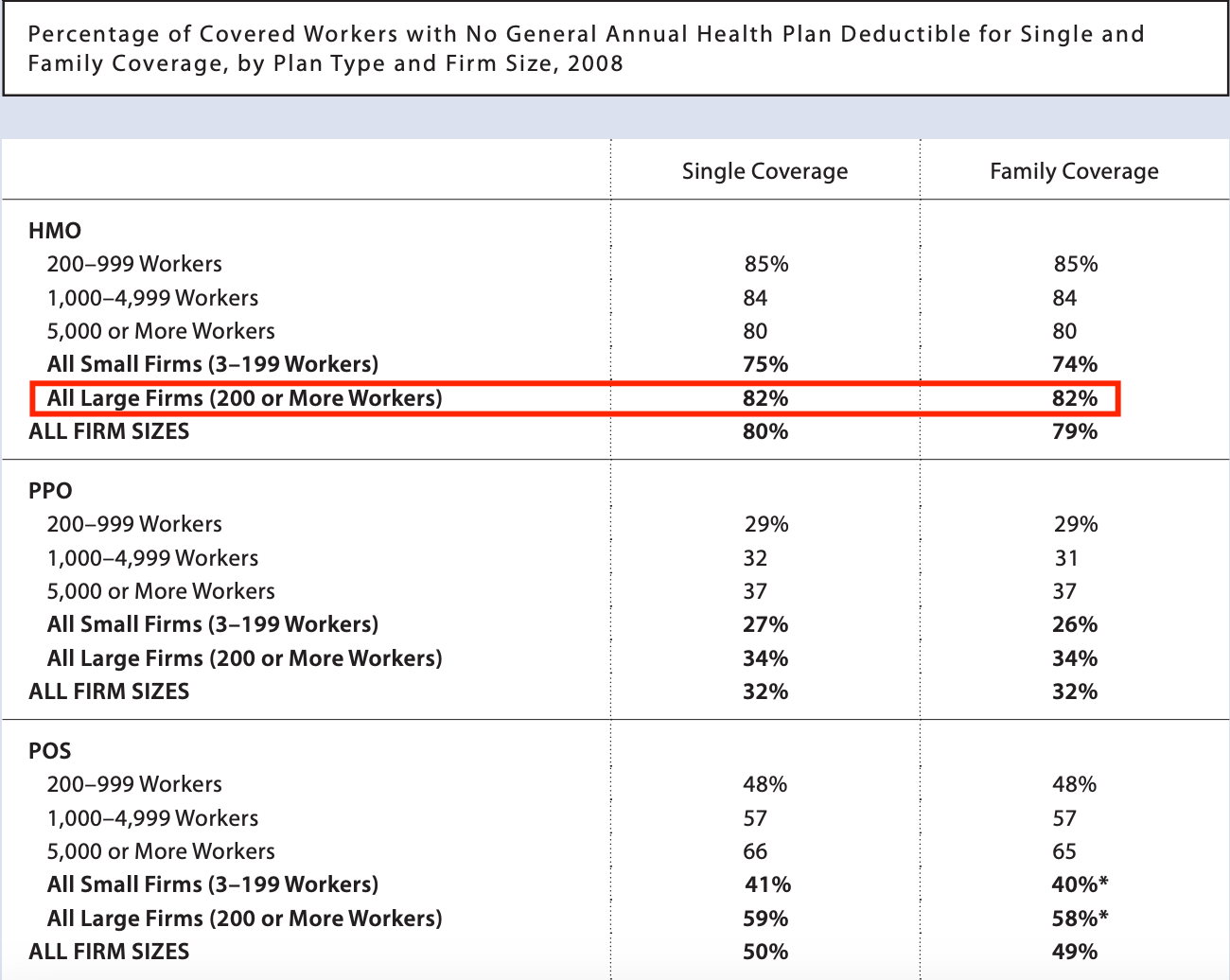

So Walter’s in-network deductible was probably $0-500, not $5,000.
In 2025, Albuquerque Public Schools offers an EPO through Blue Cross Blue Shield of New Mexico with:
$1,000 annual deductible (single)
$5,000 annual out-of-pocket maximum for medical (single)
$3,000 annual out-of-pocket maximum for prescription drugs (single)
Separate Express Scripts pharmacy benefit


Chemoradiation is billed through the medical benefit: 20% coinsurance after deductible, but once he hits the $5,000 OOP max, everything else is free that year.
Osimertinib would be a specialty drug under the pharmacy benefit. It costs about $70,000-100,000+ per year at list price. But Walter would pay:
Monthly copay of ~$125-200 (specialty tier)
Until he hits the $3,000 annual Rx OOP max
After which: $0
Many employer plans also have manufacturer copay assistance programs that reduce the effective member cost even below the stated copay, while still counting the spending toward the OOP maximum.3
The Bill
Year 1 (diagnosis, chemoradiation, start targeted therapy):
Medical OOP max: $5,000
Pharmacy OOP max: $3,000
Total: $8,000
Years 2-3 (ongoing osimertinib):
Surveillance imaging and checkups probably don’t hit the medical OOP max
Pharmacy OOP max: $3,000/year
Total: ~$3,000-4,000 per year
Three-year total: roughly $14,000-20,000 in out-of-pocket costs, excluding premiums.
So Would He Cook Meth?
Now let’s talk about what Walter actually needed the money for. He makes $43,700 a year teaching chemistry, plus car wash wages. He has a $107,000 mortgage, a $30,000 home equity line, a son with cerebral palsy, and a baby on the way. In the episode “Seven Thirty-Seven,” he sits down and calculates his family’s needs: pay off the house ($137,000), college for both kids (~$400,000), living expenses after he’s gone ($200,000+). Total: $737,000.
So the question isn’t “can he afford $14,000 in cancer bills?” It’s more like, “can he leave three-quarters of a million dollars to his family?” And the answer to that is… not legally, no.
But on the narrower question -- can he actually afford his cancer treatment? -- a teacher making $43,700/year, with access to credit, home equity, and family, can find $14,000-20,000 over three years. It would be stressful. He’d carry credit card debt. Maybe they’d skip Flynn’s college fund contributions for a while, or sell the Aztek early (addition by subtraction). But “we need $15,000 over three years for medical bills” does not naturally lead to “therefore I will manufacture methamphetamine.”
The show’s original pitch was: dying man with huge medical bills turns to crime. In 2025, he’s probably not dying, and the bills are manageable.
But was it ever really about the money?
The show’s genius is that it gives Walter a sympathetic inciting incident --cancer, family, bills -- and then slowly reveals this was never about the money. It’s about pride! Resentment! The life he thinks he should have had! His former friends offer to pay for everything in Season 1, and he refuses. He keeps cooking long after he has “enough.” When Skyler asks how much is enough, he says “more.”
Vince Gilligan has said Walter’s arc is “Mr. Chips to Scarface.” The cancer is the catalyst, but it’s *not* the cause.
The Pitch Meeting (in 2025)
So here’s your prestige TV remake:
Walter gets stage IIIA lung adenocarcinoma, EGFR-positive. His doctor tells him:
“This is serious, but with osimertinib after chemoradiation, we’re seeing patients in your situation live five, ten years or more. Insurance will cover it - you’ll have some out-of-pocket costs, probably a few thousand dollars a year.”
Walter goes home. Does he:
(A) Feel relief, accept the treatment, continue teaching chemistry, become a survivor, end credits, no show
(B) Feel rage that his life’s work amounts to a few thousand dollars he doesn’t have, remember the Nobel Prize his research contributed to, recall his former friends are billionaires, see an opportunity in the drug trade that has nothing to do with hospital bills, and start cooking meth for reasons he doesn’t fully admit to himself
The honest answer is that the 2025 version would just be a different show. The original Breaking Bad used cancer-driven desperation as the premise. In 2025, Gilligan would need to do more work to explain why a man with a serious-but-manageable chronic illness and capped healthcare costs would decide to risk everything. Walter’s situation, if it happened in 2025, would be less Greek tragedy and more character study.
Which… to be fair… is what it always was. The cancer and the bills were never really the point. They were just the excuse Walter gave himself, and us.
But try pitching that to AMC: “It’s about a chemistry teacher with good insurance who cooks meth because he’s sad.”
Doesn’t quite have the same ring to it.
Not medical or financial advice. Do not cook methamphetamine. Do get your lung nodules checked. Osimertinib is approved by the FDA for unresectable stage III EGFR-mutated NSCLC after chemoradiation based on the LAURA trial. The views expressed here are my own and not those of any employer, although honestly who else would claim them.
Numbers vary by ancestry. The Lung Cancer Mutation Consortium, which was mostly Caucasian in background, lists EGFR as the plurality of driver mutations found in never-smokers with NSLC (eTable 6)
You might be squinting your eyes at 33% as baseline 5y OS for stage III NSLC when earlier I said it was around 10-15%. Well as it turns out, this is not a mistake -- there is selection bias for “fitter” patients in clinical trials as opposed to real world data. Take that as you will.
I always thought this at the time the show first ran - he’s a teacher so yeah his pay kind of sucks but one thing he probably does have is decent health insurance that will cover standard treatment, life insurance, and a pension that will pay out to his family when he dies. “American health care is so bad he literally has no choice but to cook meth” never made sense, despite that being how a lot of universal healthcare proponents wanted to read it.
But to the show’s credit, it never says that it does! They leave plenty of clues that Walt isn’t *really* just doing this for the cancer treatment. Heck they lay it right out there when his old now rich college buddy offers to pay the bill. Money solved! But it wounds his pride, so he’d rather sell drugs.
My favorite aspect of Breaking Bad is White's HMO is absolutely correct in what it does and does not cover: the experimental treatment + surgery does not work, the cancer comes back, and he has no appreciable extension of his life expectancy.